
Why Sterile Compounding Bottlenecks Are Usually Workflow Problems
There are many reasons sterile compounding facilities hit a ceiling on output. When throughput stalls, the most common response is often to invest in more space, more equipment, or more headcount. But in practice, the root cause is not always solely a lack of resources. More often, workflow clarity, sequencing, utilization, and documentation design also contribute to the constraint.
At Restore Health Consulting, we work with licensed sterile compounding pharmacies to identify and eliminate the inefficiencies that quietly cap production. Most sterile compounding constraints are not single-point bottlenecks. In many cases, the largest gains come from sequencing, utilization alignment, and reducing non-value-added transitions between controlled environment steps.
In the case study below, we helped one facility achieve an approximately 16-fold increase in sterile compounding output, without adding a single cleanroom suite or major capital equipment.
Client Case Study: Approximately 16-Fold Increase In Sterile Compounding Capacity
A licensed sterile compounding pharmacy engaged Restore Health Consulting after struggling with persistent production bottlenecks and compliance concerns. The facility prepared compounded sterile preparations (CSPs) from non-sterile bulk pharmaceutical ingredients and excipients, but inefficiencies in its day-to-day operations were limiting output and threatening long-term scalability. The limitation wasn't demand. Performance was constrained by workflow design, changeover sequencing, and cleanroom utilization.
Results described in this case study were specific to this facility’s starting conditions, staffing model, equipment configuration, product mix, and implementation discipline. Similar results should not be assumed without a site-specific assessment.
The Starting Point
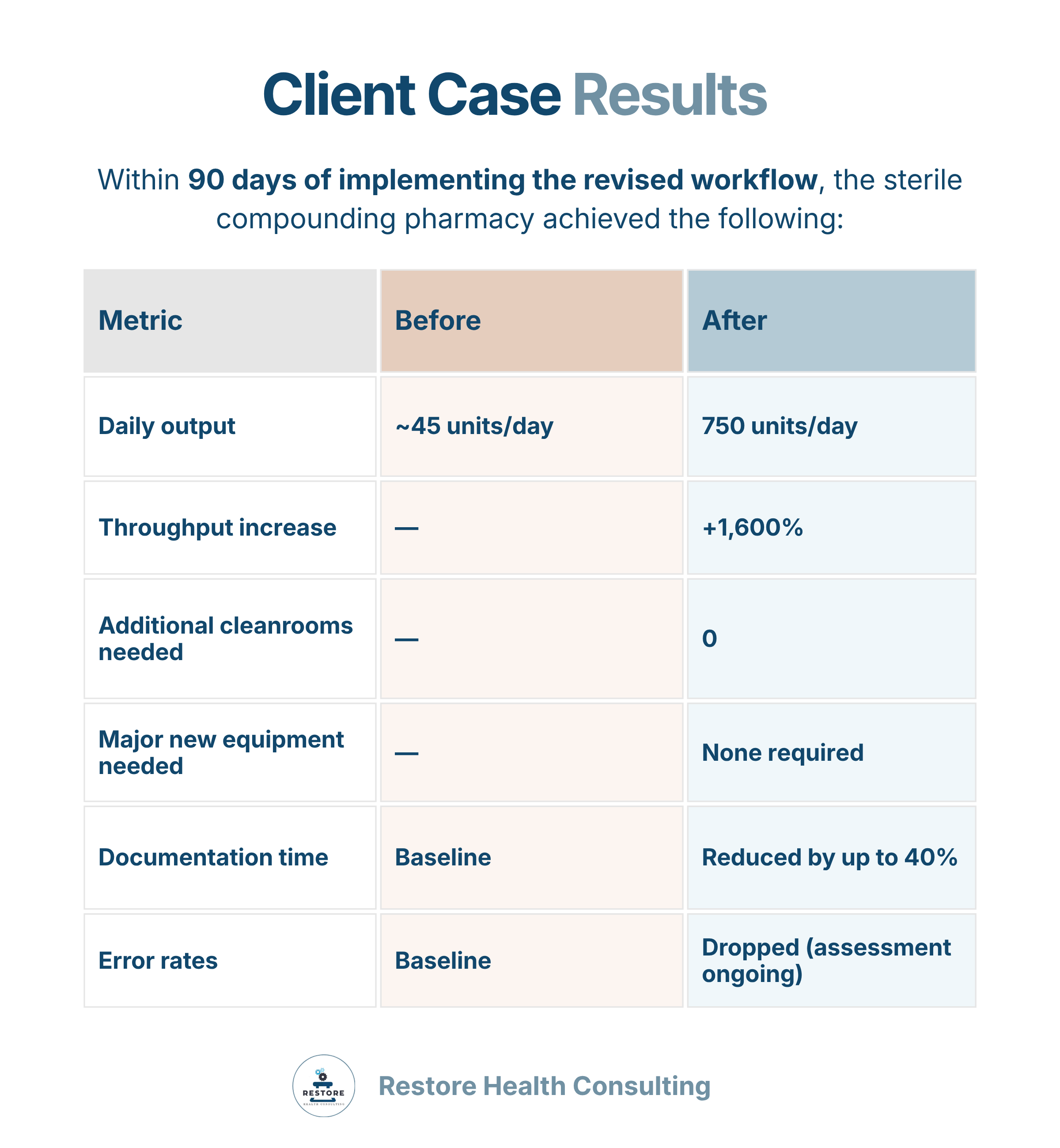
Before our engagement, the pharmacy was producing approximately 90 sterile units every other day, or roughly 45 units per day, despite having the physical infrastructure to support significantly higher throughput.
The core problems were operational, not structural:
Manual, time-consuming processes with frequent changeovers that introduced variability and reduced quality.
Inefficient material and personnel flow funneled through a single cleanroom suite.
Underutilization of available controlled environments that sat idle while bottlenecks formed elsewhere.
No standardized workflows or production sequencing, leaving each batch dependent on individual judgment rather than defined process.
What We Did
Restore Health Consulting performed a comprehensive operational and facility workflow assessment. Our approach covered five key areas:
1. Process Mapping: We identified every step in the compounding and setup process and separated value-added activities from non-value-added ones. This gave us a clear picture of where time was being lost and where interventions would have the highest impact.
2. Environmental Utilization: We evaluated air classifications, pressure differentials, and operator flow patterns to understand how the physical environment was being used, and where it wasn't being used at all. The goal was to maximize productivity within the existing single buffer/ante room configuration.
3. Equipment Optimization: Rather than recommending new equipment purchases, we redesigned workstation layout around the existing laminar airflow workbench (LAFW) and powder containment hood. The focus was on reducing idle time and minimizing unnecessary cleanroom re-entry, two of the most common hidden time sinks in sterile compounding operations.
4. Personnel and SOP Alignment: We revised training protocols and compounding SOPs to standardize setup, cleaning, and documentation sequences. This reduced transition time between compounds and eliminated the variability that came from staff improvising steps that should have been defined.
5. Scheduling Strategy: We implemented a sequencing model that brought environmental monitoring, setup, and production tasks into continuous, non-overlapping blocks. This prevented the start-stop patterns that had been fragmenting the production day.
The Results
Equipment used throughout: one buffer room, one ante room, one LAFW, two balances, one powder hood, one pump, and one crimper. Upgrades to the powder hood, balances, and pump were elective, not required, to achieve these results.
The facility’s workflow changes were designed to align with applicable State Board of Pharmacy regulations and USP <797> standards throughout the optimization process, and the site was prepared for NABP accreditation during the engagement (accreditation was achieved in the months that followed). In tandem with throughput improvements, we supported the site in implementing Category 3-aligned garbing, cleaning, and environmental monitoring controls.
Access the full case study, authored by Amy Summers, PharmD, BCSCP, FAPC, the CEO of Restore Health Consulting: https://mailchi.mp/restorehealthconsulting/16x-increase-in-sterile-compounding-capacity-case-study
7 Ways to Increase Sterile Compounding Capacity
Based on our work with sterile compounding pharmacies, here are the highest-leverage interventions for increasing output that may be achievable without major capital investment, depending on the facility’s current configuration and constraints:
1. Map your current process before changing anything. You can't optimize what you haven't measured. A thorough process map documenting every step, handoff, wait, and re-entry is the foundation of any real efficiency improvement. It's also frequently eye-opening. Most facilities discover significant time losses in steps they had never formally examined.
2. Identify your true constraint. In most compounding operations, one step determines the pace of everything else. That constraint might be in setup, in documentation, in cleaning, or in equipment access. Improving steps that aren't the constraint won't increase throughput, it will only create inventory at the bottleneck. Find the constraint and focus your energy there first.
3. Standardize setup and teardown sequences. Inconsistent setup and cleaning routines are among the most common causes of lost time between batches. When each compounder approaches setup differently, every changeover takes a different amount of time, and the average drifts upward. Standardized SOPs with defined sequences eliminate this variability and make training far more efficient.
4. Redesign workstation layout for flow. Many sterile compounding workstations are configured the way they were initially set up, not the way they'd be designed if someone started from scratch with throughput in mind. Rethinking the physical arrangement of tools, supplies, and documentation relative to the LAFW can reduce unnecessary movement and repeated cleanroom re-entries, which add time and risk.
5. Separate value-added from non-value-added steps. Not all time spent in a cleanroom is productive time. Waiting for materials, searching for supplies, re-performing undocumented steps, and correcting documentation errors are all forms of waste embedded in the production process. Once identified, many of these can be eliminated or moved outside the controlled environment entirely.
6. Implement a structured scheduling model. Ad hoc scheduling, where the day's sequence of tasks is determined informally or reactively, introduces gaps and conflicts that accumulate over time. A defined sequencing model that aligns environmental monitoring, preparation, production, and cleaning into non-overlapping blocks creates a predictable production day and prevents tasks from stepping on each other.
7. Invest in documentation systems before adding production capacity. It may seem counterintuitive, but documentation inefficiency is frequently a production bottleneck. Batch records that are poorly designed, redundant, or disconnected from the compounding process slow down both the compounder and the verifying pharmacist. Structured batch record templates with in-process checks can reduce documentation time significantly while improving traceability and reducing error rates, as demonstrated in our case study above.
How Workflow Optimization Can Improve CSP Throughput
The principles behind the results in our case study come from Lean Six Sigma, a methodology originally developed in manufacturing that has direct application in regulated pharmacy compounding environments.
At its core, Lean identifies and eliminates waste: any activity that consumes resources without adding value. In sterile compounding, waste takes many forms: unnecessary motion, waiting, defects, overprocessing, and underutilized environmental capacity. Six Sigma adds a focus on variation, which means identifying the sources of inconsistency that cause quality and throughput to fluctuate unpredictably.
When applied systematically to a sterile compounding operation, these principles routinely surface gains that are not visible to people working within the existing system. The pharmacists and technicians inside the process are often highly skilled and hard-working. However, the issue is that the process itself is designed around assumptions that were never tested.
Workflow optimization does not have to compromise quality or compliance when it is designed and implemented appropriately. In fact, the relationship typically runs in the opposite direction: standardized processes reduce error, predictable documentation reduces omissions, and consistent environmental practices support regulatory compliance.
The broader point is that regulatory standards and operational efficiency are built around related principles: consistency, control, documentation, and repeatability. A well-optimized workflow should support, rather than compete with, a compliant workflow. The friction between them usually comes from poorly designed processes, not from the demands of compliance itself. The pharmacy in our case study implemented workflow changes designed to align with USP <797> expectations and NABP accreditation readiness during the optimization process, not after it.
Common Causes of Sterile Compounding Bottlenecks
If your facility is producing below its potential, one or more of the following may be contributing:
Undefined or inconsistent SOPs. When procedures exist only informally, execution varies by individual. Batch-to-batch inconsistency emerges, and the time required for any given step becomes unpredictable.
Cleanroom re-entry. Every time a compounder leaves and re-enters a buffer room, time is lost and contamination risk increases. Facilities that haven't mapped their material and personnel flow often discover that re-entries are far more frequent than necessary.
Sequential rather than parallel scheduling. When environmental monitoring, setup, and production are scheduled one after another rather than in optimized overlapping or sequential blocks, large portions of the production window go unused.
Documentation bottlenecks. Poorly structured batch records and in-process documentation slow down both production and verification. If pharmacists are spending disproportionate time reviewing and correcting records, throughput at the final verification step becomes a constraint.
Underutilized controlled environments. Facilities often have ante rooms, pass-throughs, or secondary spaces that are not integrated into the production workflow. These assets can often be leveraged to support staging, preparation, or documentation activities that currently happen inside the buffer room.
Equipment layout misaligned with workflow. When tools, supplies, or reference materials are not positioned to support the natural sequence of compounding steps, operators compensate with additional movement and improvised workarounds, both of which cost time and introduce risk.
Reactive rather than proactive scheduling. When the day's production sequence is determined by what orders arrive rather than by a structured plan, the compounding operation can never reach its throughput ceiling because the workflow is constantly being interrupted and reorganized.
FAQ
Do we need to expand our cleanroom to increase output? Not necessarily. Our case study demonstrates that dramatic throughput increases are achievable within an existing single buffer/ante room configuration. The first step is always a thorough workflow assessment. Many facilities have substantially more capacity than their current operations are accessing.
How long does it take to see results from workflow optimization? Results vary depending on the scope of changes and the facility's starting point. In the case study above, the pharmacy achieved its full 16X throughput increase within 90 days of implementing the revised workflow.
Will optimization affect our compliance status? When done correctly, workflow optimization supports compliance rather than threatening it. Standardized SOPs, structured batch records, and defined environmental monitoring schedules all align with the expectations of USP <797>, State Board of Pharmacy regulations, and NABP accreditation. Our approach keeps compliance central throughout any operational change.
Is Lean Six Sigma applicable to sterile compounding? Yes. While Lean Six Sigma originated in manufacturing, its core principles (like eliminating waste, reducing variation, and improving flow) apply directly to regulated pharmacy compounding. The constraints of a sterile environment actually make systematic workflow design more important, not less, because the cost of inefficiency is higher and the margin for improvisation is narrower.
What's the first step if we think we have a throughput problem? Start with a process map. Document every step in your current compounding and setup workflow, including changeovers, cleaning, documentation, and environmental monitoring. Quantify the time each step takes and identify where delays, waits, and re-work are occurring. That map will tell you more about where your capacity is going than any other single exercise.
Can workflow optimization reduce documentation errors? Yes. Structured batch record templates with built-in in-process checks reduce both the time required to complete documentation and the frequency of errors that require correction. In our case study, documentation time was reduced by up to 40%, and error rates dropped as well. We continue to recommend site-specific tracking to assess long-term impact.
Ready to Find Out Where Your Capacity Is Going?
If your facility is producing below its potential, the answer may not be more space or more equipment. It's almost always in how work is moving (or not moving) through the environment you already have.
Restore Health Consulting offers a free introductory consultation to help you identify where your operation may be losing capacity and what a structured workflow assessment could uncover. There's no obligation, and no assumptions about what the solution looks like before we've looked at the problem.
Restore Health Consulting, LLC specializes in operational and regulatory compliance consulting for the personalized medicine industry. This article is intended for educational and informational purposes only and does not constitute legal, regulatory, or professional pharmacy advice. Pharmacy operations should be evaluated individually, and all workflow changes should be implemented in accordance with applicable state and federal regulations, USP standards, and accreditation requirements. Results described in this case study reflect a specific client engagement and are not guaranteed to be replicable in all settings.